Who Is Egg Freezing Suitable for, and Why Has It Become So Popular?
Egg freezing is mainly considered for people who may face reduced fertility in the future, including those who are preparing for chemotherapy, radiotherapy, or certain ovarian surgeries, as well as those who are not currently ready to have children.
However, egg freezing does not guarantee pregnancy, and its success depends greatly on the person’s age at the time of egg retrieval.
You may not yet feel ready to become a mother. Perhaps you have not found the right partner, you are building your professional path, or you want greater emotional and financial stability before having children.

At the same time, you may have repeatedly heard about the “biological clock,” declining ovarian reserve, or egg freezing. Social media sometimes presents the procedure as though a single treatment cycle can permanently remove all concerns about future fertility.
The reality is more complex.
Egg freezing can provide an important fertility-preservation opportunity for some people, but it is not necessary for everyone and cannot guarantee the birth of a baby in the future.
It only preserves the possibility of using eggs retrieved at a younger age. It does not stop all the effects that ageing may have on the body and pregnancy.
What Is Egg Freezing?
In egg freezing, also known as oocyte cryopreservation, the ovaries are stimulated using hormonal medication so that several eggs develop during one cycle instead of only one.
The eggs are then retrieved from the ovaries through a medical procedure. Mature eggs are frozen using a rapid-freezing method called vitrification and stored for possible future use.
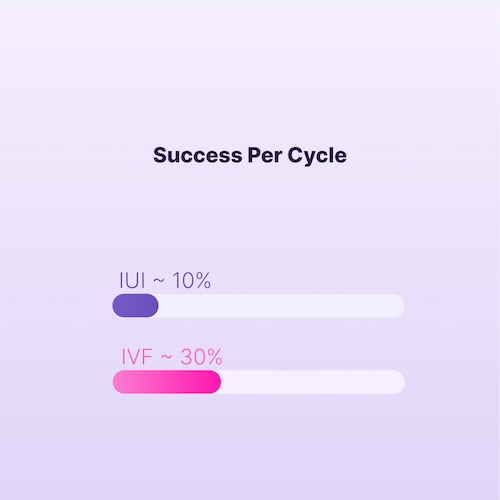
When the individual decides to pursue pregnancy, the eggs are thawed. The eggs that survive are fertilised with sperm, and if suitable embryos develop, an embryo is transferred into the uterus through IVF.
Advances in vitrification and laboratory fertilisation have improved egg-freezing outcomes compared with older freezing methods.
Who May Be a Candidate for Egg Freezing?
1. People Preparing to Begin Cancer Treatment
Some types of chemotherapy, pelvic radiotherapy, stem-cell transplantation, and surgery involving reproductive organs can reduce ovarian reserve or cause infertility.
In such circumstances, fertility-preservation options should ideally be evaluated before cancer treatment begins.
However, whether egg freezing is possible depends on the type of cancer, the person’s general medical condition, the amount of time available before treatment, and the opinion of the oncology team.
In some cases, embryo freezing, ovarian-tissue freezing, or another fertility-preservation method may be more appropriate.
For this reason, the decision should be made jointly by the oncology specialist and the fertility specialist.
2. People Whose Illness or Surgery May Damage the Ovaries
Egg freezing may also be considered for some people with non-cancerous conditions, particularly when the disease itself, medication, or a planned operation may reduce ovarian reserve.
This group may include:
- Some people with ovarian endometriosis
- People preparing for ovarian cyst surgery
- Those with a history of ovarian surgery
- People at risk of premature ovarian insufficiency
- People with certain genetic conditions
- Those who require treatments that may damage the ovaries
- People with a family history of early menopause
Having endometriosis or an ovarian cyst alone does not mean that egg freezing is necessary.
Age, ovarian reserve, the type and location of the condition, surgical history, and future family-building plans should all be evaluated together.
3. People Who Are Not Currently Ready to Have Children
Some people know that they would like to have children in the future but do not currently have suitable circumstances for pregnancy.
Their reasons may include:
- Not having found a suitable partner
- Not feeling emotionally ready for motherhood
- Wanting to complete their education
- Being at an important stage of their career
- Not yet having financial or family stability
- Wanting to have a second or third child at an older age
This type of egg freezing is often referred to as planned egg freezing or social egg freezing.
The American Society for Reproductive Medicine considers this choice ethically acceptable but emphasises that individuals should receive clear information about the probability of success, costs, risks, limitations, and the fertility clinic’s actual results.
4. People at Risk of Premature Ovarian Insufficiency
Some people may experience a severe decline in ovarian function earlier than expected because of genetic conditions, autoimmune diseases, family history, or medical treatments.
If a mother, sister, or another close family member has experienced early menopause, early consultation with a specialist may be helpful.
However, a family history of early menopause does not necessarily mean that the same thing will happen to the individual.
5. People Who Wish to Preserve Fertility Before Certain Hormonal Treatments
Some people who are preparing for long-term hormonal treatment or surgery involving reproductive organs may consider preserving their eggs before treatment begins.
The effects of the planned treatment and the possibility of fertility preservation should be assessed individually with the treatment team before the process starts.
6. People Who Do Not Currently Want to Create Embryos
Embryo freezing requires an egg to be fertilised with sperm.
Some people do not yet have a chosen partner or may not wish to create embryos at the present time for personal, legal, religious, or ethical reasons.
In these circumstances, freezing unfertilised eggs allows the person to postpone decisions about sperm and embryo creation until the future.
Do PCOS, Irregular Periods, or Low AMH Mean That Egg Freezing Is Necessary?
No. None of these conditions independently means that egg freezing is required.
AMH testing and antral follicle count are mainly used to estimate the remaining number of eggs and predict how the ovaries may respond to ovarian-stimulation medication.
A low AMH level may indicate that fewer eggs could be retrieved during one treatment cycle. However, it:
- Does not directly measure egg quality
- Does not predict the exact timing of menopause
- Does not independently determine the chance of natural pregnancy
- Does not mean definite infertility
ASRM emphasises that ovarian reserve is not the same as fertility itself.
AMH results should be interpreted alongside age, ultrasound findings, medical history, and future family-building goals.
What Is the Best Age for Egg Freezing?
There is no single fixed age that is best for everyone. However, age at the time of egg retrieval and freezing is one of the most important factors influencing future success.
As age increases, both the number of eggs and the likelihood that they are chromosomally healthy decrease.
For this reason, an egg frozen at a younger age generally has a greater chance of producing a healthy embryo.
HFEA data indicate that egg freezing before the age of 35 is generally associated with better outcomes than freezing at older ages.
However, ASRM emphasises that the evidence is not sufficient to identify one universal “ideal age” for everyone.
In practice:
- Before age 35: There is usually a greater likelihood of retrieving a higher number of eggs with suitable quality.
- Between ages 35 and 38: Egg freezing may still be beneficial, but the likelihood of needing more than one treatment cycle increases.
- After ages 38 to 40: Egg freezing may still be technically possible, but expectations regarding egg numbers and live-birth probability should be more realistic.
- After ages 40 to 45: Genetics, general health, healthy nutrition, moderate exercise, and the skill of the doctor may contribute to good outcomes in some cases. However, delaying egg freezing until this age carries greater uncertainty and is generally not advisable.
Age is not the only factor involved in decision-making.
A 33-year-old with low ovarian reserve may have different circumstances from a 40-year-old whose ovaries respond well to stimulation.
Why Has Egg Freezing Become So Popular?
Changes in the Timing of Family Formation
Many women postpone having children because of education, career development, financial circumstances, the absence of a suitable partner, or emotional readiness.
For this group, egg freezing may preserve part of their future reproductive options, although it is not a guaranteed substitute for pregnancy at a younger age.
Improvements in Freezing Technology
Vitrification has improved egg survival after thawing and fertilisation outcomes compared with older freezing methods.
This technological progress helped egg freezing move from an experimental method to a recognised fertility-preservation option.
Increased Awareness of Age-Related Fertility Decline
Information about ovarian reserve, AMH, and age-related fertility decline is now discussed more frequently in the media and on social platforms.
This greater awareness can be useful, but it may also create unnecessary fear or pressure, particularly when egg freezing is marketed as a guaranteed “fertility insurance policy.”
Greater Independence in Reproductive Planning
Egg freezing allows a person to preserve part of their future fertility options without needing a partner or making an immediate decision about embryo creation.
A Genuine Increase in Demand
Data from the United Kingdom’s fertility regulator show that the number of egg-freezing cycles increased from 2,567 cycles in 2019 to 6,932 cycles in 2023.
The greatest increase was seen among people aged 30 to 37.
However, the number of people who return to use their frozen eggs is much lower than the number of those who freeze eggs.
This shows that the growing number of egg-freezing cycles does not necessarily translate into future use or the birth of a baby.
Egg Freezing in Gulf Countries: Between Lifestyle Changes and Cultural Considerations
In recent years, egg freezing has become more visible in public conversations and specialised fertility services across Gulf countries, particularly in the United Arab Emirates and Saudi Arabia.
Changes in the timing of marriage and parenthood, continued education, greater participation of women in professional careers, the development of fertility clinics, and increasing awareness of age-related fertility decline are among the factors contributing to greater interest in this procedure.
In Abu Dhabi, THIQA policy has defined coverage for social egg freezing for eligible unmarried individuals.
The services may include up to two treatment cycles and coverage for egg storage for as long as five years.
However, acceptance levels, laws, and insurance coverage are not the same across all GCC countries.
A study involving women in the Al-Qassim region of Saudi Arabia also found that awareness and attitudes towards egg freezing varied and that higher educational attainment was associated with greater knowledge of the procedure.
In Gulf societies, decision-making may be influenced not only by medical considerations but also by confidentiality, family opinions, marital status, concern about social judgement, religious beliefs, and laws governing the future use of frozen eggs.
For this reason, counselling should be medically transparent while also respecting cultural values and the laws of the country where treatment takes place.
Benefits of Egg Freezing
Preserving Eggs Retrieved at a Younger Age
The most important benefit of egg freezing is that the biological age of the egg is preserved at the time of freezing.
For example, if a person freezes eggs at age 32 and uses them at age 40, the quality of the eggs is influenced more by the age of 32 than by the age at the time of embryo transfer.
Creating an Opportunity Before Fertility-Damaging Treatment
For people preparing for chemotherapy, radiotherapy, or certain surgeries, egg freezing may help preserve the possibility of having a genetically related child in the future.
No Need for Sperm at the Time of Freezing
Unlike embryo freezing, egg freezing does not require the person to decide on a future partner or sperm source at the time of egg retrieval.
Greater Control Over Family Planning
For some people, having frozen eggs may reduce part of the pressure to marry or have children immediately.
However, this sense of reassurance is only helpful when the person understands that egg freezing does not guarantee pregnancy.
Preserving the Possibility of a Genetic Connection
If treatment succeeds, the person may be able to create an embryo using their own eggs rather than relying on donor eggs.
Disadvantages and Limitations of Egg Freezing
It Does Not Guarantee the Birth of a Baby
Not all frozen eggs survive warming.
Among the eggs that survive:
- Not all become fertilised
- Not all develop into suitable embryos
- Not all embryos implant
- Not every pregnancy leads to the birth of a baby
HFEA emphasises that the most important risk of egg freezing is that it may ultimately fail to produce the expected outcome.
More Than One Treatment Cycle May Be Needed
The number of eggs retrieved in one cycle is not the same for everyone.
Age, ovarian reserve, and the body’s response to medication influence the number of eggs obtained.
One person may collect a suitable number of eggs in one cycle, while another may need two or more cycles to reach a similar number.
No fixed number of eggs can guarantee the birth of a child, and ASRM has not recommended one universal number of eggs needed at every age.
Costs Are Not Limited to Egg Retrieval
The total cost may include:
- Initial consultations and tests
- Ovarian-stimulation medication
- Ultrasound monitoring and treatment follow-up
- Egg retrieval
- Initial freezing
- Annual storage
- Egg warming
- Laboratory fertilisation
- Embryo culture
- Embryo transfer
Before treatment begins, the clinic should be asked about the cost of the entire pathway, not only the initial freezing procedure.
Medication and Egg-Retrieval Side Effects
Ovarian-stimulation medication may cause bloating, heaviness, headache, breast tenderness, mood changes, or pelvic discomfort.
In rare cases, ovarian hyperstimulation syndrome, or OHSS, may occur.
Egg retrieval also carries limited risks, including bleeding, infection, ovarian torsion, or complications related to anaesthesia.
Emotional Pressure and Possible Regret
If fewer eggs are retrieved than expected, or if the likelihood of success was not explained clearly, the individual may experience anxiety, disappointment, or regret.
For this reason, the clinic’s actual results, the possibility of needing several cycles, and alternative options should be explained before treatment begins.
Egg Freezing Does Not Stop the Body From Ageing
Frozen eggs do not continue to age, but the individual’s body still changes over time.
Pregnancy at an older age may be associated with a higher risk of complications such as gestational hypertension, gestational diabetes, or other maternal-health concerns.
Egg freezing therefore does not remove all the risks associated with pregnancy at an older age.
Who Should Not Proceed Only Because Egg Freezing Is Trending?
Egg freezing should not be performed solely because of clinic advertising, family pressure, a single test result, or social-media content.
Further evaluation is particularly important if:
- You believe that egg freezing guarantees pregnancy
- You have become worried only because of one low AMH result
- You are currently ready for pregnancy but are postponing it without a clear reason
- The cost of treatment would create serious financial pressure
- You expect a small number of eggs to guarantee the birth of a baby
- The probability of success based on your age and circumstances has not been explained clearly
- The clinic does not provide its actual egg-survival and live-birth statistics
People without a known medical problem or fertility risk should not feel that they are “required” to freeze their eggs in order to protect their future.
What Evaluations Are Performed Before Egg Freezing?
Depending on the individual’s circumstances, a specialist may assess:
- Age
- Medical and surgical history
- Menstrual-cycle regularity
- AMH level
- Antral follicle count by ultrasound
- Family history of early menopause
- Underlying conditions
- Current medications
- Desired number of children
- Likely timing of future egg use
These assessments help estimate how the ovaries may respond, but they cannot guarantee the outcome of treatment.
Regularly recording menstrual cycles, symptoms, medication history, and test results in DLady can help you bring more organised information to your consultation with a doctor.
What Questions Should You Ask the Clinic?
Before beginning treatment, consider asking:
- Based on my age and medical circumstances, how many mature eggs are likely to be retrieved in each cycle?
- How many ovarian-stimulation cycles might I need?
- What is the survival rate of warmed eggs in your laboratory?
- What is the live-birth rate for people who froze eggs at my age?
- Are your statistics based on live birth or only on pregnancy?
- What are the costs of medication, retrieval, storage, and future use of the eggs?
- How long can the eggs remain in storage?
- What is the next step if fewer eggs are retrieved than expected?
- What laws apply to the future use of frozen eggs in this country?
- What happens to the eggs if my marital status, place of residence, or personal decision changes?
ASRM recommends that clinics provide patients with centre-specific statistics on freezing, warming, and live-birth outcomes.
However, it is important to recognise that while this process may be emotional and deeply meaningful for the patient, it is also a commercial service and a source of income for clinics.
The Role of a Partner and Male Reproductive Health
Egg freezing is only one part of a future pregnancy journey.
Sperm quality also matters for embryo creation.
Male age, tobacco use, certain diseases, medications, excess weight, prolonged heat exposure, and underlying sperm problems may affect fertilisation or embryo development.
If you are in a stable relationship and share future family-building plans, it may be useful to evaluate the reproductive health of both partners.
Egg freezing should not cause the role of sperm health and couple-based planning to be overlooked.
Ultimately, Is Egg Freezing Right for You?
For some people, egg freezing is a medically necessary intervention.
For others, it is a planned reproductive choice.
For another group, it may be an expensive intervention with limited benefit.
The following factors should be evaluated together:
- Age
- Ovarian reserve
- Medical history
- Likelihood of delaying parenthood
- Desired number of children
- Possible need for fertility-damaging treatment
- Financial capacity
- Local laws
- Willingness to accept the possibility of treatment failure
The right decision is not one made out of fear.
The right decision is based on accurate information, specialist counselling, and your personal circumstances.
With DLady, you can record cycle patterns, symptoms, test results, and reproductive-health information so that you can make better-prepared decisions about your fertility future.
Is age 35 too late for egg freezing?
No. Egg freezing at age 35 is still possible.
However, egg number and egg quality generally decline with age. More than one treatment cycle may be needed to collect a suitable number of eggs.
Individual assessment is more important than a single age threshold.
Can eggs be frozen after age 40?
It may be technically possible, but the likelihood of retrieving a sufficient number of suitable-quality eggs is lower.
Before proceeding, the individual should receive detailed counselling about the realistic chance of success, the probable number of treatment cycles, and alternative options.
A nutrient-rich, healthy diet and moderate exercise may support general health but cannot reverse age-related decline in egg quality.
How many eggs should be frozen to have one child?
There is no guaranteed number.
The number needed depends on age at retrieval, egg quality, the laboratory’s experience, and the number of children desired.
Even a high number of frozen eggs cannot guarantee the birth of a baby.
Does a low AMH mean that I should freeze my eggs immediately?
Not necessarily.
A low AMH level mainly suggests that fewer eggs may be retrieved.
The test does not independently determine egg quality or the ability to conceive naturally.
Can I become pregnant naturally after egg freezing?
Yes.
Egg freezing does not prevent natural pregnancy in the future.
Some people never use their frozen eggs because they later conceive naturally or their family-building plans change.
Is egg freezing painful?
Medication injections may be uncomfortable, and bloating or heaviness may occur during ovarian stimulation.
Egg retrieval is usually performed under sedation or anaesthesia, and mild pain or cramping may be experienced afterwards.
Is egg freezing better than embryo freezing?
Egg freezing does not require sperm and allows decisions about embryo creation to be postponed.
Embryo freezing provides more information about fertilisation and embryo development, but it requires sperm and involves legal and ethical decisions about the embryo.
The choice is highly individual.
Does egg freezing cause early menopause?
Usually not.
Stimulation medication supports eggs that were already developing during that menstrual cycle and many of which would naturally have been lost.
However, the process should always be performed under specialist supervision.